Cardiac arrhythmia during sleep is not uncommon and can be secondary to respiratory sleep disorder like obstructive sleep apnea (OSA) [1]. However, rapid eye movement (REM) sleep-related bradyarrhythmia syndrome is an unusual primary arrhythmia characterized by transient sinus arrests and atrioventricular (AV) conductance disturbances during the REM sleep [2]. It is a rare nighttime cardiac rhythm disorder, only few cases have been published in the medical literature, and never in Korean literatures. Here, we report a 36-year-old male with REM-related high degree AV block and severe OSA.
Case Report
A 36-year-old man with documented nocturnal paroxysmal bradyarrhythmia on 24-hour Holter electrocardiography (ECG) monitoring was referred to the sleep clinic for evaluation of the relationship with sleep apnea. The patient was obese (body mass index, 29.2 kg/m2 ) and suffered from gastroesophageal reflux disease. His medical history was otherwise unremarkable. The patient had experienced three episodes of vague chest discomfort and palpitation during the last 7 months. The laboratory tests including cardiac enzymes and serum electrolytes were normal. No abnormalities were detectable on a previous transthoracic echocardiogram and coronary angiography. Exercise stress test was also negative. Repeated 24-hour Holter ECG monitoring was recorded, showing several episodes of high degree AV block at the nighttime with a maximal 5.6 seconds of ventricular pause (Fig. 1). These episodes were more frequent in the second half of the night.
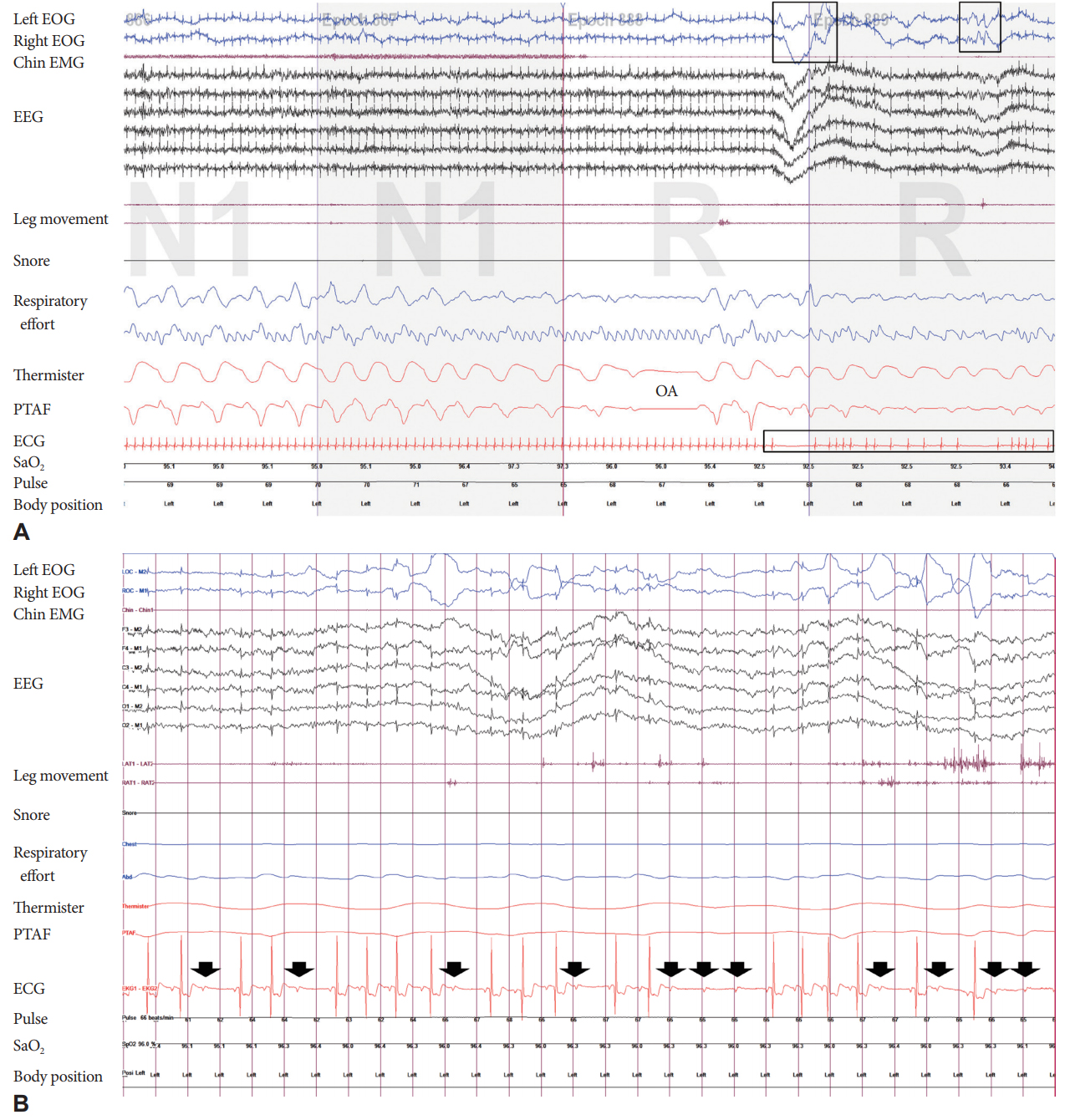
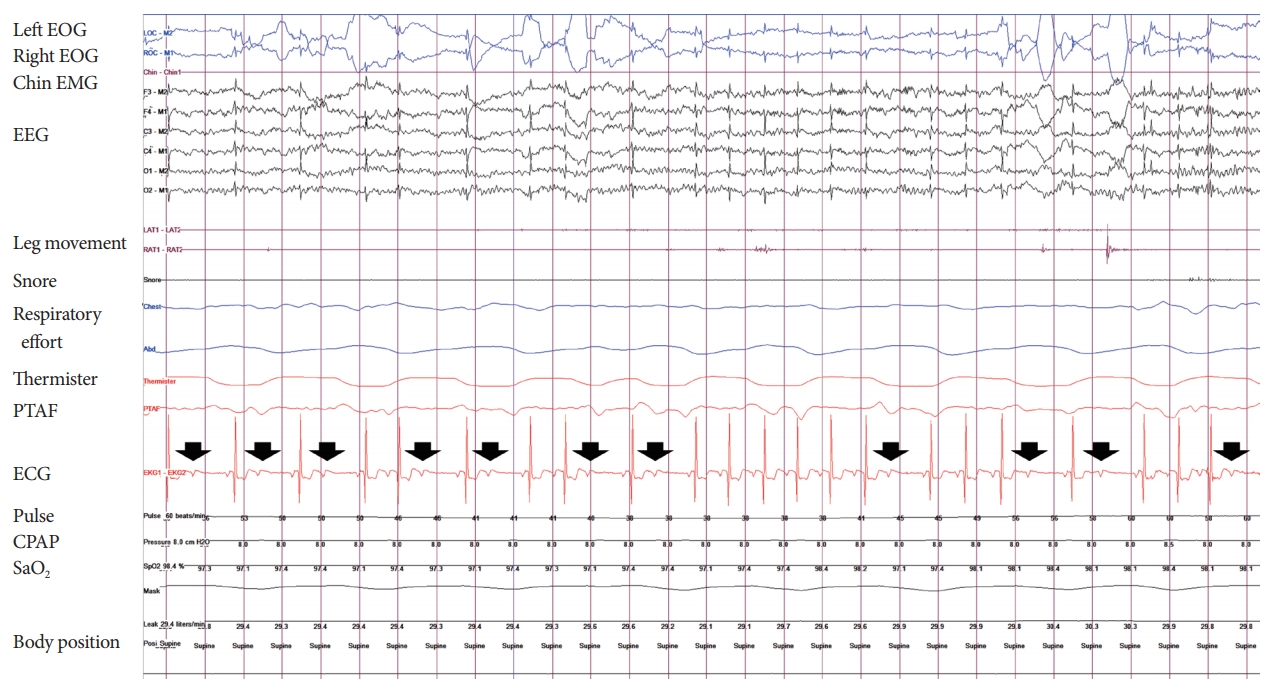
A diagnostic polysomnography (PSG) performed to investigate the relationship between sleep pattern and the cardiac arrhythmia. The PSG showed an apnea-hypopnea index (AHI) of 30.1/hour (consisting of 100% obstructive events), and the minimum oxygen saturation was 85.4%. The sleep disordered breathing was aggravated in the supine position (supine AHI 53.5/hour and non-supine AHI 9.3/hour). AHIs during REM sleep and during non-REM sleep was 40.6/hour and 27.9/hour, respectively. ECG on PSG showed 57 episodes of paroxysmal AV block only during the 71 minutes of REM sleep (with the longest pause being 5.1 seconds) (Fig. 2). There was no relationship between AV block and respiratory events. AV block occurred only during phasic REM sleep stage when bursts of REM were observed. AV block did not occur during non-REM sleep. The patient was asymptomatic during these ventricular pauses. To investigate the possibility of OSA-related arrhythmia, full-night in-laboratory continuous positive airway pressure (CPAP) titration was performed. CPAP at 8 cmH2O alleviated sleep-disordered breathing to the optimal level (overall AHI 4.9/hour and REM AHI 4.6/hour). Nevertheless, the 43 episodes of paroxysmal AV block during the 39 minutes of REM sleep were noted (Fig. 3). Therefore, REM sleep-related bradyarrhythmia was diagnosed. The CPAP treatment was started at home for severe OSA syndrome. The patient was not given specific treatment for REM sleep-related bradyarrhythmia due to a lack of accompanied significant symptoms.
Discussion
The association of various cardiac arrhythmias with OSA has been described in multiple studies [1]. These OSA-related cardiac arrhythmias showed significant resolution when treated with CPAP [3,4]. On the other hand, during REM sleep, bradyarrhythmia such as high degree AV block or sinus pause independent of sleep-disordered breathing can be observed. Since the first report by Holty & Guilleminault in 1984 [2], REM sleep-related bradyarrhythmia was known to occur only in otherwise healthy individuals, but cases with concomitant severe OSA syndrome or severe hypertension were recently reported [5,6]. Unlike OSA-related cardiac arrhythmia, REM sleep-related bradyarrhythmia did not improve by CPAP treatment [5].
Differential diagnosis between OSA-related cardiac arrhythmia and REM sleep-related bradyarrhythmia syndrome is crucial in determining the treatment strategy for the underlying disease and its complication. In some studies, apnea-associated bradyarrhythmia showed predominance during REM sleep [7]. Although at the initial PSG, the patient had AV block only during phasic REM sleep stage, we could not exclude the possibility of OSA-related arrhythmia due to his severe OSA. However, the patient’s AV block during phasic events of REM sleep continued even on optimal CPAP level. There was no specific abnormality on the other cardiac evaluation, so the patient was diagnosed with REM sleep-related AV block.
The exact mechanisms for REM-related bradyarrhythmia are still unknown. The autonomic nervous system is a fundamental modulator of cardiac rhythm. The interaction between sympathetic and parasympathetic tone determines nocturnal heart rate. These autonomic components are regulated by sleep stage cycle, body posture, sleep apnea, and arousals [8]. In general, REM sleep is characterized by sympathetic dominance and suppression of the parasympathetic tone. However, the shift to an increased low to high frequency ratio from slow wave sleep to REM sleep tended to be lower on analysis of heart rate variability in some patients with REM sleep-related bradyarrhythmia. This may reflect increased vagal activity during REM sleep [9]. Heightened vagal tone and/or abrupt cessation of sympathetic activity during phasic REM events is hypothesized to cause REM-sleep related bradyarrhythmia syndrome [2].
The clinical significance and standardized treatment for REM sleep-related bradyarrhythmia syndrome remains controversial. Numerous arrhythmias may be detected during sleep, and the majority without diurnal symptoms or clinical signs have demonstrated a benign course. The validity of the assumption that REM-related sinus arrest or AV block predisposes to sudden nocturnal cardiac death is unproven. However, some cases of REM sleep-related bradyarrhythmia syndrome are associated with significant symptoms. Therefore, consideration of pacemaker implantation is suggested for symptomatic REM-associated bradyarrhythmia syndrome [10].
In conclusion, this case highlights the existence of REM sleep-related bradyarrhythmia that is not improved by optimal CPAP level in patients with severe OSA syndrome. Hence, we believe that REM sleep-related bradyarrhythmia syndrome represents a new category of sleep-related disorder. Sleep medicine specialists have to pay attention to this syndrome because it can be diagnosed by nocturnal PSG. Further prospective study should be done to clarify the clinical course and treatment of this sleep stage specific arrhythmia.