ņä£ ļĪĀ
ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØĆ ņłśļ®┤ ņżæ ļ░śļ│ĄņĀüņØĖ ņāüĻĖ░ļÅäņØś ĒÅÉņāēņ£╝ļĪ£ ņØĖĒĢ┤ ĒśĖĒØĪņØś ņĀĆĒĢśļéś ņżæļŗ©ņØä ņĢ╝ĻĖ░ĒĢśļ®░ ņĀĆņé░ņåīņ”ØņØ┤ļéś Ļ░üņä▒ņØä ņ£Āļ░£ĒĢ£ļŗż[1]. ļśÉĒĢ£, ņŻ╝Ļ░äņĪĖļ”╝ņ”ØņØä ņ┤ēļ░£ĒĢśĻ│Ā ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś, Ļ│ĀĒśłņĢĢņØä ļ╣äļĪ»ĒĢ£ ņŗ¼ļćīĒśłĻ┤ĆĻ│ä ņ¦łļ│æ ļ░Å ļīĆņé¼ņä▒ ņ¦łĒÖśņØś ņ£äĒŚśņØĖņ×ÉņØ┤ļŗż[2]. ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØä ņ¦äļŗ©ĒĢśļŖö Ēæ£ņżĆļ░®ļ▓ĢņØĖ ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼(polysomnography, PSG)ļŖö ņĄ£ĻĘ╝ ĻĄŁļé┤ņŚÉņä£ ĻĖēņŚ¼ĒÖöĻ░Ć ņŗ£Ē¢ēļÉśņ¢┤ ĒÖśņ×ÉĻ░Ć ļČĆļŗ┤ĒĢśļŖö Ļ▓Ćņé¼ļ╣äņÜ® ņĀĆĒĢśļĪ£ ņØĖĒĢ┤ Ļ▓Ćņé¼ ņĀæĻĘ╝ļÅäļŖö ļåÆņĢäņĪīņ£╝ļéś, Ļ▓Ćņé¼ņ×ÉņøÉņØś ĒĢ£ņĀĢņ£╝ļĪ£ ņØĖĒĢ┤ ņŚ¼ņĀäĒ׳ Ļ▓Ćņé¼ņŗ£Ē¢ēĻ╣īņ¦ĆņØś ĻĖ┤ ļīĆĻĖ░ĻĖ░Ļ░äņØ┤ ņĪ┤ņ×¼ĒĢ£ļŗż. ļ¼┤ĒśĖĒØĪņØś ņ╣śļŻīļĪ£ ņ¢æņĢĢ ĒÖśĻĖ░(continuous positive airway pressure, CPAP) ņ╣śļŻīļź╝ ņäĀĒāØĒĢśļ®┤ ņ×ÉļÅÖņ¢æņĢĢĻĖ░ļź╝ ņé¼ņÜ®ĒĢśņ¦Ć ņĢŖļŖö ĒĢ£, ņøÉņ╣ÖņĀüņ£╝ļĪ£ ņ¢æņĢĢ ņĀüņĀĢ(CPAP titration)ņØä ņ£äĒĢ£ ņČöĻ░ĆņĀüņØĖ PSGĻ░Ć ĒĢäņÜöĒĢśļŗż. ĻĄŁļé┤ļ│┤ļŗż ļ©╝ņĀĆ PSGĻ░Ć ņØ╝ņ░Ź ļīĆņżæĒÖöļÉ£ ņä£ĻĄ¼ņäĀņ¦äĻĄŁņŚÉņä£ļÅä Ļ▓Ćņé¼ ļ╣äņÜ®, ņĀæĻĘ╝ņä▒, Ļ▓Ćņé¼ ņåīņÜö ņŗ£Ļ░ä ļō▒ņØś ņĖĪļ®┤ņØ┤ ņ¦äļŗ© ļ░Å ņ╣śļŻīņØś ņ×Āņ×¼ņĀüņØĖ ņĀĆĒĢ┤ņÜöņåīļĪ£ ņ×æņÜ®Ē¢łļŹś ļ░ö, ĒĢśļŻ╗ļ░żņØś PSGņŚÉņä£ ņ¦äļŗ©Ļ│╝ ņ╣śļŻīļź╝ ļÅÖņŗ£ņŚÉ ĒĢśļŖö ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼(split-night PSG)ņØś ņé¼ņÜ®ņØä ĻČīņןĒĢśĻ│Ā ņ׳ļŗż[3,4]. ņ┤łĻĖ░ ļ»ĖĻĄŁņłśļ®┤ĒĢÖĒÜīņŚÉņä£ļŖö ņĄ£ņåī 2ņŗ£Ļ░ä ļÅÖņĢł PSG Ļ▓Ćņé¼ņŚÉņä£ ļ¼┤ĒśĖĒØĪ-ņĀĆĒśĖĒØĪņ¦Ćņłś(apnea-hypopnea index, AHI)Ļ░Ć ņŗ£Ļ░äļŗ╣ 40ĒÜī ņØ┤ņāüņØś ĒÖśņ×É ļśÉļŖö AHIĻ░Ć 20ĒÜī ņØ┤ņāüņØ┤ļ®┤ņä£ ņ¢æņĢĢņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢśļŗżĻ│Ā ĒīÉļŗ©ļÉśļŖö Ļ▓ĮņÜ░, ņłśļ®┤ Ēøäļ░śĻĖ░ņŚÉ ņ¢æņĢĢ ņĀüņĀĢņØä ņŗ£Ē¢ēĒĢĀ ņłś ņ׳ļŗżĻ│Ā ĒĢśņśĆņ£╝ļéś, ņĄ£ĻĘ╝ņŚÉļŖö AHIĻ░Ć 15ĒÜī ņØ┤ņāüņØĖ Ļ▓ĮņÜ░ļĪ£ ĻĘĖ ņĀüņÜ® ļ▓öņ£äļź╝ ļäōĒ×ī ļ░ö ņ׳ļŗż[4,5]. ĒĢśņ¦Ćļ¦ī ņØ┤ ĻĘ╝Ļ▒░ļŖö ņŻ╝ļĪ£ ņä£ĻĄ¼ņŚÉņä£ ņ¦äĒ¢ēļÉ£ ņŚ░ĻĄ¼ņŚÉ ĻĖ░ļ░śņØä ļæÉņ¢┤ ļÅÖņ¢æņØĖņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņŚ░ĻĄ¼Ļ▓░Ļ│╝ļŖö ļČĆņĪ▒ĒĢ£ ĒśäņŗżņØ┤ļŗż[6-9]. ĒĢ£ĻĄŁņØĖņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ ņŗ£ņ×æ Ēøä 2ņŗ£Ļ░ä ļÅÖņĢłņØś AHIņÖĆ ņĀäņ▓┤ AHIņØś ņØ╝ņ╣śņ£©ņØ┤ ļåÆļŗżļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆļŗż. ĒĢśņ¦Ćļ¦ī ņØ┤ ņŚ░ĻĄ¼ļŖö ņĀäņ▓┤ ļīĆņāü 150ļ¬ģ ņżæ ļé©ņä▒ņØ┤ 123ļ¬ģņ£╝ļĪ£ ļé©ņä▒ņØś ļ╣äņ£©(82%)ņØ┤ ņŚ¼ņä▒ņŚÉ ļ╣äĒĢ┤ ņøöļō▒Ē׳ ļåÆņĢśĻ│Ā, ļö░ļĪ£ ņŚ¼ņä▒ ņ¦æļŗ©ņŚÉņä£ļ¦ī AHIņØś ņØ╝ņ╣śļÅäļź╝ ļ╣äĻĄÉĒĢ£ Ļ▓░Ļ│╝ļŖö ņŚåņŚłļŗż[10]. ņŚ¼ņä▒ņØ┤ ļÅÖņØ╝ĒĢ£ ņ▓┤ņ¦łļ¤ēņ¦ĆņłśņØś ļé©ņä▒ļ│┤ļŗż ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØś ņżæņ”ØļÅäĻ░Ć ļŹ£ĒĢśļ®░, NREMņłśļ®┤ņŚÉ ļ╣äĒĢ┤ REMņłśļ®┤ ņżæ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØ┤ ļŹö ņŗ¼ĒĢśļŗżļŖö Ļ▓āņØä Ļ│ĀļĀżĒĢśļ®┤, ļé©ņä▒ņżæņŗ¼ņØś ņŚ░ĻĄ¼ņŚÉņä£ ļÅäņČ£ĒĢ£ Ļ▓░Ļ│╝ļź╝ ņŚ¼ņä▒ņŚÉĻ▓ī ĻĘĖļīĆļĪ£ ņĀüņÜ®ĒĢśļŖö Ļ▓āņØ┤ ļ¼┤ļ”¼ņØ╝ ņłś ņ׳ļŗż[11-13]. ļ│Ė ņŚ░ĻĄ¼ļŖö ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪ ņ¦äļŗ©ņØä ņ£äĒĢ┤ PSGļź╝ ņŗ£Ē¢ēĒĢ£ ņŚ¼ņä▒ļ¦īņØä ļīĆņāüņ£╝ļĪ£ 2ņŗ£Ļ░ä ļÅÖņĢłņØś AHIņÖĆ ņĀäņ▓┤ AHIņØś ņØ╝ņ╣śļÅäļź╝ ĒÖĢņØĖĒĢśĻ│Āņ×É ĒĢśņśĆļŗż.
ļ░® ļ▓Ģ
ļ│Ė ņŚ░ĻĄ¼ļŖö ļČĆņé░ ņ¦ĆņŚŁņØś ĒĢ£ ļīĆĒĢÖļ│æņøÉ ņłśļ®┤Ēü┤ļ”¼ļŗēņŚÉņä£ 2011ļģä 11ņøö~2019ļģä 6ņøöĻ╣īņ¦Ć ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØä ņØśņŗ¼ĒĢ┤ PSGļź╝ ņŗ£Ē¢ēĒĢ£ ņä▒ņØĖ ņŚ¼ņä▒ ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ Ē¢łļŗż. ņ×ÉļŻīņłśņ¦æņØä ņ£äĒĢ┤ ļČĆņé░ļ░▒ļ│æņøÉ ņ£żļ”¼ņŗ¼ņØśņ£äņøÉĒÜīņØś ņŖ╣ņØĖņØä ļ░øņĢśĻ│Ā(IRB No. 202012-046), ĒøäĒ¢źņĀü ņØśļ¼┤ĻĖ░ļĪØ ņĪ░ņé¼ņŚ░ĻĄ¼ļĪ£ ļÅÖņØś ņłśņ¦æņØĆ ļ®┤ņĀ£ļÉÉļŗż.
ņŚ░ĻĄ¼ ļīĆņāü
ņĮöĻ│©ņØ┤ņÖĆ ļ¼┤ĒśĖĒØĪņØä ņŻ╝ņåīļĪ£ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØ┤ ņØśņŗ¼ļÉśņ¢┤ PSGļź╝ ņŗ£Ē¢ēĒĢ£ 18ņäĖ ņØ┤ņāüņØś ĒĢ£ĻĄŁņØĖ ņä▒ņØĖļé©ņä▒ņØä ņĀ£ņÖĖĒĢ£ ņŚ¼ņ×É 133ļ¬ģņØä ļīĆņāüņ£╝ļĪ£ Ē¢łļŗż. 1) PSGņŚÉņä£ AHIĻ░Ć ņŗ£Ļ░äļŗ╣ 5ĒÜī ļ»Ėļ¦ī, 2) ņłśļ®┤ņ×Āļ│ĄĻĖ░(sleep latency)Ļ░Ć 90ļČä ņØ┤ņāü, 3) ņżæņČöņä▒ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪ(central apneaŌēź5/h), 4) ĒīīņØ╝ ņåÉņāüņ£╝ļĪ£ PSG ņøÉļ│ĖņØä ĒÖĢņØĖĒĢĀ ņłś ņŚåļŖö Ļ▓ĮņÜ░ļŖö ļČäņäØļīĆņāüņŚÉņä£ ņĀ£ņÖĖĒĢśņśĆļŗż.
ņŚ░ĻĄ¼ ļÅäĻĄ¼
ņĢ╝Ļ░ä ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼(Full-night polysomnography, FN-PSG)
PSGļŖö Remlogic(Embla Systems, Denver, CO, USA)ņ£╝ļĪ£ ņŗ£Ē¢ēĒ¢łļŗż. ņłśļ®┤ ļŗ©Ļ│äņÖĆ Ļ░üņä▒ņØś ĒīÉņĀĢņØĆ ļćīĒīī(C3-A2, C4-A1, F3-A2, F4-A1, O3-A2, O2-A1), ņĢłņĀäņ£äļÅä(electrooculography), Ēä▒ ĻĘ╝ņĀäļÅä(chin electromyography)ļĪ£ Ē¢łļŗż. ņś©ļÅäĻ░Éņ¦Ćņä╝ņä£ņÖĆ ņĢĢļĀźņä╝ņä£ļĪ£ ĒśĖĒØĪļ¤ēņØä ņĖĪņĀĢĒĢśņśĆĻ│Ā, ĒØēĻ│ĮĻ│╝ ļ│ĄļČĆļ▓©ĒŖĖļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ĒśĖĒØĪņÜ┤ļÅÖņØä ņĖĪņĀĢĒ¢łļŗż. ĻĘĖ ņÖĖ ļ¦źļ░Ģņé░ņåīņĖĪņĀĢ(pulse oximetry), ņŗ¼ņĀäļÅä, ņ¢æņ¬Į ņĢ×ņĀĢĻ░ĢĻĘ╝(tibialis anterior muscle)ņØś ĻĘ╝ņĀäļÅäņÖĆ ņ▓┤ņ£äļź╝ ņĖĪņĀĢĒ¢łĻ│Ā, Ļ▓Ćņé¼ ņĀä Ļ│╝ņĀĢņØĆ ļ╣äļööņśżļĪ£ ĻĖ░ļĪØĒ¢łļŗż. PSG ļŗ╣ņØ╝ņŚÉļŖö ņłśļ®┤ņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö ņĢīņĮöņś¼ņØ┤ļéś ņ╣┤ĒÄśņØĖņØ┤ ĒĢ©ņ£ĀļÉ£ ņØīļŻīļź╝ ļ│ĄņÜ®ĒĢśņ¦Ć ņĢŖļÅäļĪØ Ē¢łļŗż.
ņłśļ®┤ ļŗ©Ļ│ä, ĒśĖĒØĪņé¼Ļ▒┤ ļ░Å Ļ░üņä▒ ļō▒ņŚÉ ļīĆĒĢ£ ĒīÉļÅģņØĆ ļ»ĖĻĄŁ ņłśļ®┤ĒĢÖĒÜīņØś ņ¦Ćņ╣©ņŚÉ ļö░ļ×Éļŗż[14]. ļ¼┤ĒśĖĒØĪ(apnea)ņØĆ 10ņ┤ł ņØ┤ņāü ĒśĖĒØĪņØ┤ ļ®łņČöĻ▒░ļéś, ļ╣äĻ░ĢņØś ņś©ļÅäņÖĆ ņĢĢļĀźņä╝ņä£ļź╝ ĒåĄĒĢ┤ Ļ│ĄĻĖ░ĒØÉļ”äņØ┤ 90% ņØ┤ņāü Ļ░ÉņåīĒĢśļŖö Ļ▓ĮņÜ░, ņĀĆĒśĖĒØĪ(hypopnea)ņØĆ 10ņ┤ł ņØ┤ņāü Ļ│ĄĻĖ░ĒØÉļ”äņØ┤ 30% ņØ┤ņāü Ļ░ÉņåīņÖĆ ņé░ņåīĒżĒÖöļÅäĻ░Ć 3% ņØ┤ņāü ļ¢©ņ¢┤ņ¦ĆĻ▒░ļéś Ļ░üņä▒ņØä ļ│┤ņØ╝ ļĢīļĪ£ ĒĢśņśĆļŗż[14]. ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØĆ AHIĻ░Ć 5/h ņØ┤ņāüņØĖ Ļ▓ĮņÜ░ļĪ£ ņĀĢņØśĒ¢łļŗż.
ņäżļ¼Ėņ¦Ć
ņäżļ¼Ėņ¦ĆļŖö ņłśļ®┤ Ēü┤ļ”¼ļŗēņŚÉ ņ▓śņØī ļ░®ļ¼ĖĒĢ£ ļéĀ ņ×æņä▒ļÉśņŚłļŗż.
ņŚĪņøīņŖżņĪĖņØīņ▓ÖļÅä(Epworth Sleepiness Scale)
ņŻ╝Ļ┤ĆņĀüņØĖ ņŻ╝Ļ░ä ņĪĖļ”╝ņ”Ø(daytime sleepiness)ņØś ņĀĢļÅäļź╝ ļéśĒāĆļé┤ļŖö ņ▓ÖļÅäļĪ£, 8Ļ░Ćņ¦Ć ņāüĒÖ®ņŚÉņä£ ņ×ĀņØ┤ ļōż ņłś ņ׳ļŖö Ļ░ĆļŖźņä▒ņØä 0(ņĀłļīĆ ņĪĖņ¦Ć ņĢŖņØī)ņŚÉņä£ 3(ņĪĖ Ļ▓ā Ļ░ÖņØī) ļ▓öņ£äļĪ£ ĒÅēĻ░ĆĒĢ£ļŗż. ņ┤ØņĀÉ 0~24ņĀÉņØ┤ļŗż. ņĀÉņłśĻ░Ć Ēü┤ ņłśļĪØ ņĪĖļ”╝ņ”ØņØ┤ ņŗ¼ĒĢśĻ│Ā, 10ņĀÉ ņØ┤ņāüņØ┤ļ®┤ Ļ│╝ļÅäĒĢ£ ņŻ╝Ļ░äņĪĖļ”╝(excessive daytime sleepiness)ņØ┤ ņ׳ņØīņØä ņØśļ»ĖĒĢ£ļŗż[15].
ļ▓Ī ņÜ░ņÜĖ ņ▓ÖļÅä(Beck Depression Inventory-II)
ņ¦Ćļé£ 2ņŻ╝Ļ░ä ņÜ░ņÜĖĒĢ©ņØś ņĀĢļÅäļź╝ ņĖĪņĀĢĒĢśļŖö Ļ▓āņ£╝ļĪ£ 21Ļ░Ćņ¦Ć ĒĢŁļ¬®ņ£╝ļĪ£ ĻĄ¼ņä▒ļÉ£ļŗż. ņ┤ØņĀÉņØĆ 0~63ņĀÉņØ┤ļ®░, ņĀÉņłśĻ░Ć Ēü┤ ņłśļĪØ ņÜ░ņÜĖĒĢ©ņØä ļ£╗ĒĢ£ļŗż. ĒĢ£ĻĄŁņØĖņØä ļīĆņāüņ£╝ļĪ£ ņ×äņāüņĀüņ£╝ļĪ£ ņØśļ»Ėņ׳ļŖö ņÜ░ņÜĖ ņ”ØņāüņØś ņ┤ØņĀÉ ņĀłļŗ©Ļ░Æ(cutoff value)ņØĆ 17ņĀÉņØ┤ļŗż[16].
ņ×ÉļŻī ļČäņäØ
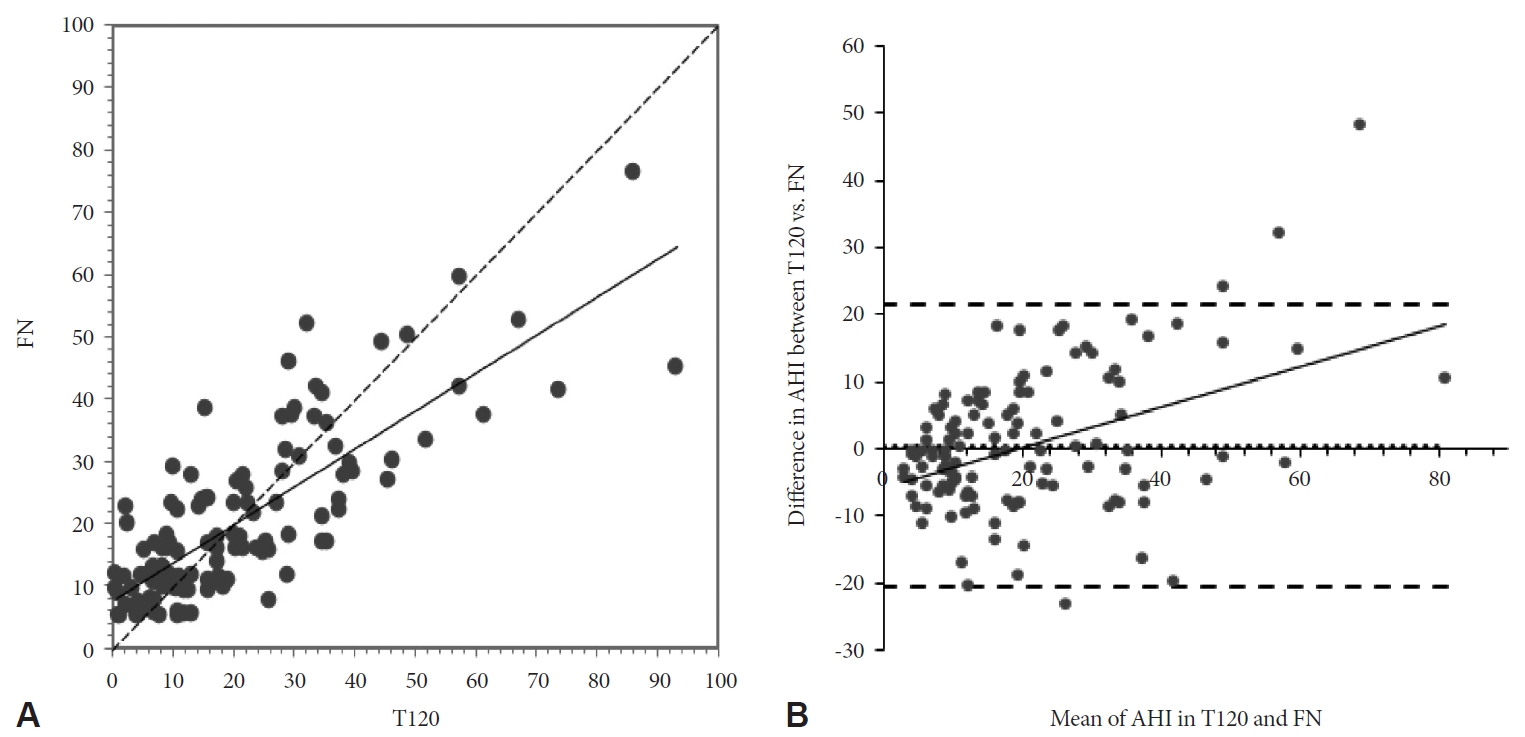
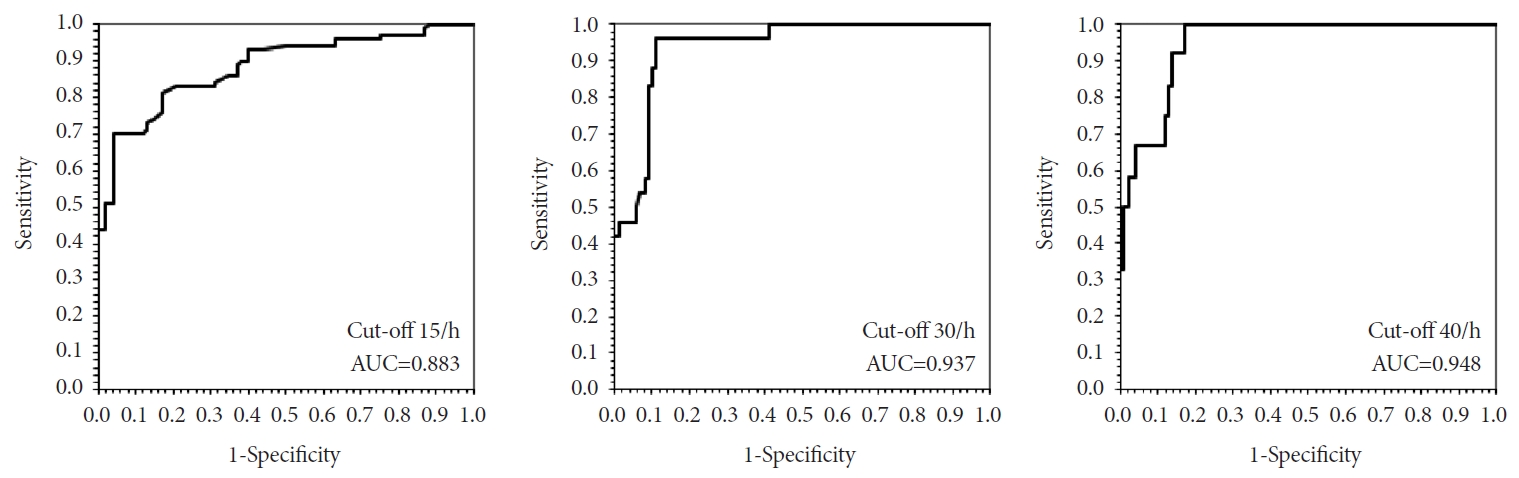
FN-PSGņØś AHIļź╝ ĻĖ░ņżĆĻ░Æņ£╝ļĪ£ ņ×ĪĻ│Ā, Ļ▓Ćņé¼ļź╝ ņ£äĒĢ┤ ļČłņØä ļüł ņŗ£ņĀÉņØä PSG Ļ▓Ćņé¼ ņŗ£ņ×æņŗ£Ļ░äņ£╝ļĪ£ ņäżņĀĢĒĢśĻ│Ā, 120ļČä ļśÉļŖö 90ļČä Ļ▓ĮĻ│╝ ņŗ£ņĀÉņØś AHI(T120-AHI, T90-AHI)ņÖĆ ņØ╝ņ╣śļÅäļź╝ ļ│┤ņĢśļŗż. ņØ╝ņ╣śļÅäņØś ĒīÉņĀĢņØĆ ņØ╝ņ╣śņä▒ ņāüĻ┤ĆĻ│äņłś(concordance correlation coefficient, CCC)ņÖĆ ļĖöļ×£ļō£-ņĢ©ĒŖĖļ©╝ ļÅäĒæ£(Bland-Altman plot)ļź╝ ņØ┤ņÜ®ĒĢśņśĆļŗż. FN-AHIņŚÉ ļīĆĒĢ£ T120-AHIĻ│╝ T90-AHIņØś ņ¦äļŗ©ņĀü ļ»╝Ļ░ÉļÅä ļ░Å ĒŖ╣ņØ┤ļÅäļź╝ ņĢīņĢäļ│┤ĻĖ░ ņ£äĒĢ┤ Ļ░üĻ░ü 15/h, 30/h, 40/hņØś ņĀłļŗ©Ļ░ÆņŚÉ ļīĆĒĢśņŚ¼ receiver operating characteristics (ROC) curveļź╝ ĒÖĢņØĖĒ¢łļŗż. ņŚ░ļĀ╣ļīĆļ│ä FN-AHIņÖĆ T120-AHIĻ░äņØś ņ£ĀņØśĒĢ£ ņ░©ņØ┤Ļ░Ć ņ׳ļŖöņ¦Ć ņĢīņĢäļ│┤ĻĖ░ ņ£äĒĢ┤ ņ£īņĮĢņŖ© ļČĆĒśĖ ņł£ņ£äĻ▓ĆņĀĢ(WilcoxonŌĆÖs signed ranks test)ņØä ņØ┤ņÜ®ĒĢśņśĆļŗż.
Ļ▓░ Ļ│╝
ņŚ░ĻĄ¼ ļīĆņāü 133ļ¬ģ ņżæ 11ļ¬ģņØ┤ ņäĀņĀĢĻĖ░ņżĆņŚÉņä£ ĒāłļØĮĒĢśņŚ¼, ņä▒ņØĖ ņŚ¼ņä▒ 122ļ¬ģņØś Ļ▓░Ļ│╝ļź╝ ļČäņäØĒĢśņśĆļŗż.
ņØ╝ļ░śņĀü ĒŖ╣ņä▒ ļ░Å ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ Ļ▓░Ļ│╝
ĒÖśņ×ÉļōżņØś ļéśņØ┤, ņ▓┤ņ¦łļ¤ēņ¦Ćņłś, ļ¬®ļæśļĀłļź╝ ĒżĒĢ©ĒĢ£ ņØĖĻĄ¼ĒĢÖņĀü ņä▒Ļ▓®Ļ│╝ ņäżļ¼Ė ļ░Å PSG Ļ▓░Ļ│╝ļŖö Table 1Ļ│╝ Ļ░Öļŗż. ņłśļ®┤ņ×Āļ│ĄĻĖ░, ļĀśņłśļ®┤ ņ×Āļ│ĄĻĖ░ņØś ĒÅēĻĘĀĻ░ÆņØĆ Ļ░üĻ░ü 12.1ļČä, 120.2ļČäņØ┤ņŚłļŗż. 122ļ¬ģņØĆ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØś ņżæņ”ØļÅäņŚÉ ļö░ļØ╝, Ļ▓Įņ”Ø 56ļ¬ģ, ņżæļō▒ļÅä 42ļ¬ģ, ņżæņ”Ø 24ļ¬ģņ£╝ļĪ£ ļČäļźśļÉśņŚłļŗż. ņĢÖņÖĆņ£ä(supine)ņÖĆ ļĀśņłśļ®┤ņŗ£ AHIĻ░Ć ņ”ØĻ░ĆĒĢśļŖö ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż.
T120-AHIņÖĆ FN-AHIņØś ņØ╝ņ╣śļÅä
ņØ╝ņ╣śņä▒ ņāüĻ┤ĆĻ│äņłśļź╝ ņØ┤ņÜ®ĒĢ£ T120-AHIņÖĆ FN-AHIļŖö ņ£ĀņØśĒĢ£ ņłśņżĆņØś ņØ╝ņ╣śļÅäļź╝ ļ│┤ņśĆļŗż(CCC=0.773)(Fig. 1A). ļĖöļ×£ļō£-ņĢ©ĒŖĖļ©╝ ļÅäĒæ£ņŚÉņä£ļŖö, T120-AHIņÖĆ FN-AHI ņ░©ņØ┤Ļ░ÆņŚÉ ļīĆĒĢ£ ĒÅēĻĘĀņØĆ 0.46ņ£╝ļĪ£ 0ņŚÉ Ļ░ĆĻ╣īņÜ┤ Ļ░ÆņØä ļ│┤ņśĆļŗż(Fig. 1B). T120-AHIņŚÉņä£ AHIņØś ņĀłļŗ©Ļ░Æ 15, 30, 40ņØä ņé¼ņÜ®ĒĢ£ ROC ņ╗żļĖī ņĢäļלņØś ļ®┤ņĀü(area under the curve, AUC)ņØĆ ļ¬©ļæÉ ņ£ĀņØśĒ¢łņ£╝ļ®░, Ļ░üĻ░üņØś ļ»╝Ļ░ÉļÅäņÖĆ ĒŖ╣ņØ┤ļÅäļŖö ņĀłļŗ©Ļ░Æ 15ņØ╝ ļĢī 78.6%, 82.7%, 30ņØ╝ ļĢī 79.2%, 90.8%, 40ņØ╝ ļĢī 66.7%, 96.4% ņśĆļŗż(Fig. 2).
T90-AHIņÖĆ FN-AHIņØś ņØ╝ņ╣śļÅä
ņØ╝ņ╣śņä▒ ņāüĻ┤ĆĻ│äņłśļź╝ ņØ┤ņÜ®ĒĢ£ T90-AHIņÖĆ FN-AHIņŚÉņä£ļÅä ņ£ĀņØśĒĢ£ ņłśņżĆņØś ņØ╝ņ╣śļÅäļź╝ ļ│┤ņśĆļŗż(CCC=0.739)(Supplementary Fig. 1A in the online-only Data Supplement). ļĖöļ×£ļō£-ņĢ©ĒŖĖļ©╝ ļÅäĒæ£ņŚÉņä£ļŖö, T90-AHIņÖĆ FN-AHI ņ░©ņØ┤Ļ░ÆņØś ĒÅēĻĘĀņØĆ 0.02ļĪ£ 0ņŚÉ Ļ░ĆĻ╣īņÜ┤ Ļ░ÆņØä ļ│┤ņśĆļŗż(Supplementary Fig. 1B in the online-only Data Supplement). T90-AHIņŚÉņä£ AHIņØś ņĀłļŗ©Ļ░Æ 15, 30, 40ņØä ņé¼ņÜ®ĒĢ£ AUC Ļ░ÆņØĆ ļ¬©ļæÉ ņ£ĀņØśĒ¢łņ£╝ļ®░, Ļ░üĻ░üņØś ļ»╝Ļ░ÉļÅäņÖĆ ĒŖ╣ņØ┤ļÅäļŖö ņĀłļŗ©Ļ░Æ 15ņØ╝ ļĢī 77.1%, 86.5%, 30ņØ╝ ļĢī 66.7%, 87.8%, 40ņØ╝ ļĢī 58.3%, 93.6% ņśĆļŗż(Supplementary Fig. 2 in the online-only Data Supplement).
Ļ│Ā ņ░░
ļ│Ė ņŚ░ĻĄ¼ļŖö ĒĢ£ĻĄŁ ņä▒ņØĖ ņŚ¼ņä▒ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪ ĒÖśņ×ÉņŚÉņä£ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ¦äļŗ©ņĀü ņØśņØśļź╝ ņĢīņĢäļ│┤ĻĖ░ ņ£äĒĢśņŚ¼, T120-AHIņÖĆ FN-AHIļź╝ ļ╣äĻĄÉĒĢśņśĆĻ│Ā, T120-AHIņØś ņ¦äļŗ©ņĀü ņ£ĀņÜ®ņä▒ņØä ņ×ģņ”ØĒĢśņśĆļŗż. ņØ┤ļŖö ņØ┤ņĀä ņŚ░ĻĄ¼Ļ▓░Ļ│╝ļōżņŚÉņä£ ņŚ¼ņä▒ņØ┤ ļé©ņä▒ņŚÉ ļ╣äĒĢ┤ ņāüļīĆņĀüņ£╝ļĪ£ ļ╣äļĀśņłśļ®┤ AHIĻ░Ć ļé«Ļ│Ā, ļ╣äļĀśņłśļ®┤ AHIņÖĆ ļĀśņłśļ®┤ AHIņØś ņ░©ņØ┤Ļ░Ć ņŗ¼ĒĢśņŚ¼[11-13], ļé©ņä▒ņŚÉ ļ╣äĒĢ┤ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ¦äļŗ©ņĀü ņĀĢĒÖĢļÅäĻ░Ć ļ¢©ņ¢┤ņ¦ł Ļ▓āņØ┤ļØ╝ļŖö ņśłņāüĻ│╝ļŖö ļŗżļźĖ Ļ▓░Ļ│╝ņśĆļŗż. Won ļō▒ņØĆ 2057ļ¬ģņØś ļŹ░ņØ┤Ēä░ļź╝ ņé¼ņÜ®ĒĢ£ ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£, ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪ ĒÖśņ×ÉņØś ņä▒ļ│äņŚÉ ļö░ļØ╝ PSG Ļ▓░Ļ│╝ļź╝ ļ╣äĻĄÉĒ¢łņØä ļĢī, ņĀäņ▓┤ AHI Ļ░ÆņØĆ ļé©ņä▒ņŚÉņä£ ļåÆĻ│Ā, ĒŖ╣Ē׳ ļ╣äļĀśņłśļ®┤ AHI Ļ░ÆņØś ņ░©ņØ┤Ļ░Ć ņŗ¼ĒĢśļéś, ļĀśņłśļ®┤ AHIļŖö ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖļŖöļŗżĻ│Ā ĒĢśņśĆļŗż[12]. Zhang ļō▒ņØĆ ļé©ņä▒ļ│┤ļŗż ņŚ¼ņä▒ņŚÉņä£ ņāüļīĆņĀüņ£╝ļĪ£ ļĀśņłśļ®┤ AHIĻ░Ć ļåÆĻ│Ā, ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ ļ╣äļĀśņłśļ®┤ AHIļŖö ļé«ņØĆ Ļ▓░Ļ│╝ļź╝ ļ│┤Ļ│ĀĒĢśņśĆļŗż[13]. ļśÉĒĢ£ ļæÉ ņŚ░ĻĄ¼ ļ¬©ļæÉņŚÉņä£ ļé©ņä▒ļ│┤ļŗż ņŚ¼ņä▒ņØś ļĀśņłśļ®┤ ņ×Āļ│ĄĻĖ░Ļ░Ć ĻĖĖņŚłļŗż[12,13]. ļ╣äņŖĘĒĢ£ ņ▓┤ņ¦łļ¤ēņ¦ĆņłśņØś ļé©ņä▒ņØ┤ ņŚ¼ņä▒ļ│┤ļŗż ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØś ņĀĢļÅäĻ░Ć ņŗ¼ĒĢśĻ│Ā, ļé©ņä▒ņŚÉņä£ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØś ņ£Āļ│æļźĀņØ┤ ļåÆņØĆ ņøÉņØĖņØĆ ņĢäņ¦ü ļ¬ģĒÖĢĒ׳ ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśņ£╝ļéś, ņ¦Ćļ░®ņØś ļČäĒż, ņāüĻĖ░ļÅäņØś ĒĢ┤ļČĆĒĢÖņĀü ĻĄ¼ņĪ░, ĒśĖĒØĪ ņĪ░ņĀł, ĒśĖļź┤ļ¬¼, ļģĖĒÖö ļō▒ņØś ņŚ¼ļ¤¼Ļ░Ćņ¦Ć ņĖĪļ®┤ņŚÉņä£ ņ░©ņØ┤Ļ░Ć ņ׳ĻĖ░ ļĢīļ¼ĖņØ┤ļØ╝Ļ│Ā ņŚ¼Ļ▓©ņ¦ĆĻ│Ā ņ׳ļŗż[17]. ņāüĻĖ░ļÅäņØś ĻĄ¼ņĪ░ņŚÉņä£, ļé©ņä▒ņŚÉņä£ ļŹö ĻĖĖĻ│Ā ļŖśņ¢┤ņ¦ä(floppy) ĻĄ¼ņØĖļæÉļź╝ Ļ░Ćņ¦ĆĻ│Ā, ļŹö Ēü¼Ļ│Ā ņ¦Ćļ░®ņØ┤ ļ¦ÄņØĆ ĒśĆļź╝ Ļ░Ćņ¦ĆĻ│Ā ņ׳ņ£╝ļ®░[17], ļéśņØ┤Ļ░Ć ļōżļ®┤ņä£, ņŚ¼ņä▒ņŚÉ ļ╣äĒĢ┤ ļé©ņä▒ņŚÉņä£ Ēä▒ļüØĒśĆĻĘ╝ņØś ņØīņĢĢņŚÉ ļīĆĒĢ£ ļ░śņØæņØ┤ ļ¢©ņ¢┤ņ¦Ćļ®┤ņä£, ĻĖ░ļÅäĻ░Ć ĒÅÉņćäļÉśĻĖ░ ņēĮļŗż[18]. ļśÉĒĢ£ ļ╣äļĀśņłśļ®┤ņŚÉņä£ ņāüĻĖ░ļÅä ņĀĆĒĢŁņØ┤ ņ”ØĻ░ĆĒĢśņśĆņØä ļĢī, ņ×Éļ░£ņĀü Ļ░üņä▒ ņØ┤Ēøä ņŚ¼ņä▒ņŚÉ ļ╣äĒĢ┤ ņĀĆĒÖśĻĖ░ļÉśĻ│Ā ĻĖ░ļÅä ĒÅÉņćäņä▒(collapsibility)ņØ┤ ņ”ØĻ░ĆĒĢśļŖö ļō▒ņØś Ļ░üņä▒ ņØ┤Ēøä ļ░£ņāØĒĢśļŖö ņāüĻĖ░ļÅäņØś ļČłņĢłņĀĢņä▒ņ£╝ļĪ£ļÅä ņØ╝ļČĆ ņäżļ¬ģĒĢśĻ│Ā ņ׳ļŗż[12,19-21]. ņä▒ĒśĖļź┤ļ¬¼ņØś ņŚŁĒĢĀļÅä ņŻ╝ņÜöĒĢśĻ▓ī ņŚ¼Ļ▓©ņ¦ĆļŖöļŹ░, ĒÅÉĻ▓Į ņØ┤ņĀäņŚÉ ļ╣äĒĢ┤ ĒÅÉĻ▓ĮĻĖ░ ļ░Å ĒÅÉĻ▓ĮĻĖ░ ņØ┤Ēøä AHIĻ░Ć ĻĖēĻ▓®Ē׳ ļåÆņĢäņ¦ĆĻ│Ā, ĒÅÉĻ▓ĮĻĖ░ ņØ┤ĒøäņØś ņŚ¼ņä▒ņŚÉņä£ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØś ņ£Āļ│æļźĀņØ┤ ļåÆļŗż[22-24]. ņØ┤ļ¤¼ĒĢ£ ĒÅÉĻ▓ĮĻĖ░ ņĀäĒøäļĪ£ņØś ĻĖēĻ▓®ĒĢ£ ļ│ĆĒÖöļŖö ņŚÉņŖżĒŖĖļĪ£Ļ▓ÉĻ│╝ ĒöäļĪ£Ļ▓īņŖżĒģīļĪĀņØ┤ ĒÖśĻĖ░ļź╝ ņ×ÉĻĘ╣ĒĢśĻ│Ā ņāüĻĖ░ļÅäļź╝ ĒÖĢņןĒĢśļŖö ņ×æņÜ®ņØä ĒĢśņŚ¼, ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņŚÉ ņĀĆĒĢŁņĀüņØĖ ņ×æņÜ®ņØä ĒĢĀ Ļ▓āņØ┤ļØ╝ļŖö ņŚ░ĻĄ¼Ļ▓░Ļ│╝ļōżņØ┤ ņ׳ņ£╝ļéś, ĻĘĖ ĻĖ░ņĀäņØ┤ ņĢäņ¦ü ļ¬ģĒÖĢĒ׳ ļ░ØĒśĆņ¦Ćņ¦ĆļŖö ņĢŖņĢśļŗż[24,25]. ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö, ĒÅÉĻ▓Į ņØ┤Ēøä ņŚ¼ņä▒ņŚÉņä£ ĒśĖļź┤ļ¬¼ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņØä ņŗ£ ņŗ£Ē¢ēĒĢśļŖö ĻĄ░ļ│┤ļŗż ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØś ņ£äĒŚśļÅäĻ░Ć 4ļ░░ ņØ┤ņāü ņ”ØĻ░ĆĒĢ£ļŗżĻ│Ā ļ░£Ēæ£Ē¢łļŗż[26]. ļśÉĒĢ£ ņłśņłĀ Ēøä ļ░£ņāØĒĢ£ ĒÅÉĻ▓ĮņŚÉņä£, ņŚÉņŖżĒŖĖļĪ£Ļ▓É/ĒöäļĪ£Ļ▓īņŖżĒģīļĪĀ ļ│ĄĒĢ® ĒśĖļź┤ļ¬¼ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢ£ Ēøä AHIĻ░Ć Ļ░ÉņåīĒ¢łļŗżļŖö ņŚ░ĻĄ¼Ļ▓░Ļ│╝ļÅä ņ׳ņŚłļŗż[22]. ĒÅÉĻ▓Į ņØ┤Ēøä ĒśĖļź┤ļ¬¼ņØś ļ│ĆĒÖöļĪ£, ņŚ¼ņä▒ņŚÉņä£ ļ¬ĖĒåĄņØś ņ¦Ćļ░®ņØ┤ ņ”ØĻ░ĆĒĢśņŚ¼, ļé©ņä▒ņØś ņ¦Ćļ░®ļČäĒżņÖĆ Ļ░ÖņØ┤ ļ│ĆĒÖöĒĢśļŖö Ļ▓ā ļśÉĒĢ£ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØś ņŻ╝ņÜö ņ£äĒŚśņØĖņ×ÉļĪ£ ļ░ØĒśĆņ¦ĆĻ│Ā ņ׳ļŗż[27,28].
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļÅä, ļĀśņłśļ®┤ AHIĻ░Ć ļ╣äļĀśņłśļ®┤ AHIļ│┤ļŗż ļåÆņĢśĻ│Ā ĒÅēĻĘĀ ļĀśņłśļ®┤ ņ×Āļ│ĄĻĖ░ļŖö 120.2ļČä, T120ņŚÉ ļĀśņłśļ®┤ņØ┤ ņ׳ņŚłļŹś ĒÖśņ×ÉĻ░Ć 60ļ¬ģ, ĻĘĖ ņżæ ņĢÖņÖĆņ£ä ļĀśņłśļ®┤ņØ┤ ĒżĒĢ©ļÉ£ Ļ▓ĮņÜ░ļŖö 45ļ¬ģņØ┤ņŚłņ£╝ļéś, T120-AHIĻ░Ć FN-AHIņÖĆ ļåÆņØĆ ņØ╝ņ╣śļÅäļź╝ ļ│┤ņśĆļŗż(Supplementary Table 1 in the online-only Data Supplement). ļ│Ė ņŚ░ĻĄ¼ļīĆņāüņØś ĒÅēĻĘĀ ņŚ░ļĀ╣ņØ┤ 57ņäĖļĪ£ ļåÆĻ│Ā, ļīĆļČĆļČä ĒÅÉĻ▓ĮĻĖ░ ņØ┤ĒøäņØś ņŚ¼ņä▒ņ×äņØä Ļ│ĀļĀżĒĢśļ®┤, ņŚ░ļĀ╣ņŚÉ ņØśĒĢ┤ ļé©ļģĆņØś AHI ņ░©ņØ┤Ļ░Ć ĒؼņäØļÉśņŚłņØä Ļ░ĆļŖźņä▒ļÅä Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗż(Supplementary Table 2 in the online-only Data Supplement).
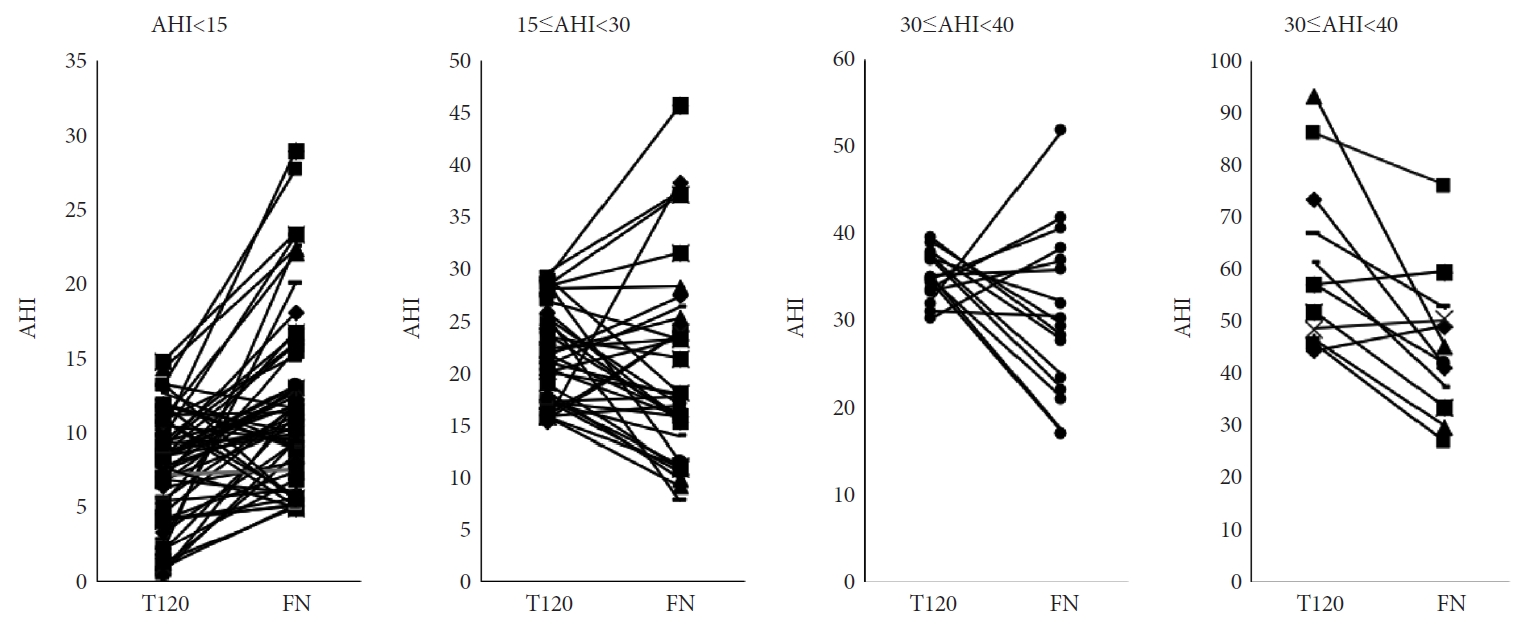
ņ▓śņØī 2ņŗ£Ļ░ä Ēś╣ņØĆ 3ņŗ£Ļ░äņØś ļÅÖņĢłņØś AHIņÖĆ, ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś AHIĻ░äņØś ļåÆņØĆ ņØ╝ņ╣śļÅäļź╝ ĒåĄĒĢ┤ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ¦äļŗ©ņĀü ņĀĢĒÖĢļÅäĻ░Ć ļåÆņØĆ Ļ▓āņØĆ ņØ┤ļ»Ė ņĢīļĀżņĀĖ ņ׳ņ£╝ļéś, ņŻ╝ļĪ£ ņä£ņ¢æņØĖļōżņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņŚ░ĻĄ¼Ļ▓░Ļ│╝ņśĆļŗż[6-9]. Kim ļō▒ņØĆ ĒĢ£ĻĄŁņØĖ ļé©ņ×É 123ļ¬ģņØä ĒżĒĢ©ĒĢ£ ĒĢ£ĻĄŁņØĖ 150ļ¬ģņØś ļŹ░ņØ┤Ēä░ļź╝ ļČäņäØĒĢ£ Ļ▓░Ļ│╝, ņ▓śņØī ļæÉņŗ£Ļ░ä ļÅÖņĢłņØś AHIņÖĆ, ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś AHIĻ░Ć ņ£ĀņØśĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŗż[10]. ļ│Ė ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤, ņŚ¼ņä▒ņØä ĒżĒĢ©ĒĢ£ ĒĢ£ĻĄŁņØĖ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪ ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ¦äļŗ©ņĀü ņØśņØśĻ░Ć ļŹöņÜ▒ ļ¬ģĒÖĢĒĢ┤ņ¦ł Ļ▓āņØ┤ļØ╝ ņāØĻ░üĒĢ£ļŗż.
ļśÉĒĢ£, T120ņŚÉņä£ AHI 15, 30, 40ņØś ņĀłļŗ©Ļ░ÆņØä ņé¼ņÜ®ĒĢśņśĆņØä ļĢī, ņĀłļŗ©Ļ░ÆņØ┤ ļåÆņĢäņ¦łņłśļĪØ ļ»╝Ļ░ÉļÅäĻ░Ć Ļ░ÉņåīĒĢśņśĆĻ│Ā, ĒŖ╣Ē׳ ņĀłļŗ©Ļ░Æ 40ņØ╝ ļĢī 66.7%ņØś ļé«ņØĆ ļ»╝Ļ░ÉļÅäļź╝ ļéśĒāĆļé┤, ņżæļō▒ļÅä ņØ┤ņāüņØś ĒÅÉņćäņłś ļ®┤ļ¼┤ĒśĖĒØĪņŚÉņä£ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ļź╝ ĻČīĻ│ĀĒĢśļŖö ņĄ£ĻĘ╝ņØś ĻČīĻ│Āņé¼ĒĢŁņØä ņ¦Ćņ¦ĆĒĢĀ ņłś ņ׳ļŖö Ļ▓░Ļ│╝ņØ┤ļŗż.
ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö, ņØ┤ņĀä ņŚ░ĻĄ¼ļōżņŚÉņä£ ļ¦ÄņØ┤ ņé¼ņÜ®ĒĢśņ¦Ć ņĢŖņØĆ, ņ▓śņØī 90ļČä ļÅÖņĢłņØś AHIņØś ņ¦äļŗ©ņĀü ņ£ĀņÜ®ņä▒ņØä ĒĢ©Ļ╗ś Ļ▓ĆĒåĀĒĢśņśĆņ£╝ļ®░, ĒØźļ»ĖļĪŁĻ▓īļÅä T90-AHIļÅä T120-AHIņÖĆ ņ£ĀņØśĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłņ£╝ļ®░, FN-AHIņÖĆ ļåÆņØĆ ņØ╝ņ╣śļÅäļź╝ ļ│┤ņśĆļŗż. ļæÉ ņŗ£Ļ░ä ļ»Ėļ¦īņØś ņ¦äļŗ©ņĀü ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ļź╝ ĒåĄĒĢ£ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ļŖö ņĢäņ¦ü ļ»Ėļ»ĖĒĢśļéś, ņØ┤ĒøäņŚÉļÅä ņØ┤ļ¤¼ĒĢ£ Ļ▓░Ļ│╝ļōżņØ┤ ļ░śļ│ĄļÉ£ļŗżļ®┤, ņČöĒøä ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ¦äļŗ©ņĀü ņłśļ®┤Ļ▓Ćņé¼ņŚÉ ņé¼ņÜ®ĒĢśļŖö ņŗ£Ļ░äņØä ņżäņØ┤Ļ│Ā, ņ¢æņĢĢ ņĀüņĀĢņŚÉ ļ░░ļČäĒĢśļŖö ņŗ£Ļ░äņØä ļŖśļĀż ņ¢æņĢĢ ņĀüņĀĢņØś ņä▒Ļ│ĄļźĀņØä ļåÆņØ┤ļŖöļŹ░ ļ│┤Ēā¼ņØ┤ ļÉĀ ņłśļÅä ņ׳ņØä Ļ▓āņØ┤ļŗż.
ļ│Ė ņŚ░ĻĄ¼ļŖö ļŗ©ņØ╝ ņāüĻĖēņóģĒĢ®ļ│æņøÉ ņłśļ®┤ņä╝Ēä░ņŚÉņä£ PSGļź╝ ņŗ£Ē¢ēĒĢ£ ņä▒ņØĖ ņŚ¼ņä▒ ĒÖśņ×Éļ¦īņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ĒøäĒ¢źņĀü ņŚ░ĻĄ¼ņØ┤ļ®░, ļ¬©ļōĀ ĒÖśņ×ÉļōżņØś ĒÅÉĻ▓Į ņŚ¼ļČĆļź╝ ļ¬ģĒÖĢĒ׳ ĒÖĢņØĖĒĢśņ¦Ć ļ¬╗ĒĢśņśĆĻ│Ā, Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢ£ ņŚ░ļĀ╣ļīĆ ļśÉĒĢ£ ļåÆņĢä, ļīĆļČĆļČäņØś ĒÖśņ×ÉĻ░Ć ĒÅÉĻ▓ĮĻĖ░ Ēś╣ņØĆ ĒÅÉĻ▓ĮĻĖ░ ņØ┤ĒøäņØś ņŚ░ļĀ╣ļīĆņŚÉ ĒĢ┤ļŗ╣ĒĢśņŚ¼ ņŚ¼ņä▒ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪ ĒÖśņ×É ņĀäņ▓┤ļź╝ ļīĆĒæ£ĒĢśņ¦Ć ļ¬╗ĒĢ£ļŗż(Supplementary Table 2 in the online-only Data Supplement).
ļśÉĒĢ£ ņä▒ņØĖ ļé©ņä▒ ļ░Å ņĀĢņāü ļīĆņĪ░ĻĄ░ņØś ļŹ░ņØ┤Ēä░Ļ░Ć ņŚåņ¢┤ ļ╣äĻĄÉĒĢĀ ņłś ņŚåņ£╝ļ®░, T120ņŚÉņä£ AHIļź╝ ņĀ£ņÖĖĒĢ£ ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ Ļ▓░Ļ│╝ļź╝ ĒĢ©Ļ╗ś ņĀ£ņŗ£ĒĢśņ¦Ć ņĢŖņĢä, T120Ļ│╝ FNņØś AHI ņØ╝ņ╣śļÅäļź╝ ļ│┤ļĀżļŖö ļ¬®ņĀüņŚÉļŖö ļČĆĒĢ®ĒĢśļéś, ĒÅŁļäōņØĆ ņĀĢļ│┤ļź╝ ņĀ£Ļ│ĄĒĢśņ¦Ć ļ¬╗ĒĢ£ ņĢäņē¼ņÜ┤ ņĀÉņØ┤ ņ׳ļŗż.
ļ│Ė ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤, ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪņØ┤ ņØśņŗ¼ļÉśļŖö ņä▒ņØĖ ņŚ¼ņä▒ņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ¦äļŗ©ņĀü ņØśņØśļź╝ ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż. ņĢ×ņ£╝ļĪ£ ņŚ¼ņä▒ ĒÅÉņćäņłśļ®┤ļ¼┤ĒśĖĒØĪ ĒÖśņ×ÉņŚÉņä£ ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ£ĀņÜ®ņä▒ņØä ņĀĢļ”ĮĒĢśĻĖ░ ņ£äĒĢ┤, ĻĘĖļ”¼Ļ│Ā ļæÉņŗ£Ļ░ä ņØ┤ļé┤ņØś ļČäĒĢĀņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ņØś ņ¦äļŗ© ļÅäĻĄ¼ļĪ£ņä£ņØś ĒÜ©ņÜ®ņä▒ņŚÉ ļīĆĒĢ£ ļŹö ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņØ┤ ĒĢäņÜöĒĢĀ Ļ▓āņØ┤ļŗż.